
Summary
The High Authority for Health (HAS) offers an updated version of the recommendations for the care of children and adolescents living with HIV.
In particular, it presents, in table form, the recommended antiretroviral treatment depending on the patient’s age, namely triple therapy comprising:
- 2 nucleoside/nucleotide reverse transcriptase inhibitors (NRTI);
- and a third antiretroviral agent including raltegravir (RAL), dolutegravir (DTG) or bictegravir (BIC) as first-line treatment.
In addition to the patient’s age, the HAS recommendations emphasize the importance of taking into account:
- the effectiveness of the treatment with respect to the infection;
- the patient’s adherence to his treatment, particularly during the transition to adolescence: whenever possible, it is recommended to adapt the treatment to lifestyle, and to seek simplification to allow good long-term compliance term ;
- the galenics and characteristics of drugs available on the market, which influence acceptability and therefore compliance.
Based on these recommendations, the HAS has developed information sheets for patients and those around them, in which it highlights the mode of transmission of HIV and the benefits of properly followed treatment.
La Haute Autorité de santé (HAS) has published an updated version of the French recommendations for the care of children and adolescents living with HIV [1, 2].
This update requested by the National AIDS Council (CNS) and the National Agency for Research on AIDS and Emerging Infectious Diseases (ANRS/MIE) was necessary to take into account the epidemiological evolution of this infection in France. and the evolution of the therapeutic arsenal for the pediatric population.
In 2024, the majority of cases of mother-to-child transmission reported in France concern children from countries with high endemicity due to lack of screening or treatment of the mother. In the adolescent population, sexual transmission now represents the majority of new cases of HIV infection in France.
These recommendations are aimed at health professionals (pediatricians, infectious disease specialists, general practitioners, virologists, nurses, psychologists, school doctors, pharmacists and maternal and child protection centers), social workers and the patients themselves.
In addition to the recommendations for good practice, HAS offers a set of educational documents:
- for children and adolescents living with HIV, and those around them: information sheets [3, 4] summarizing the essential recommendations relating to social and sexual life, and treatments. In particular, the HAS underlines the importance of optimal compliance with antiretroviral treatment:
- a treatment taken correctly is taken every day, without forgetting or stopping, preferably at the same time,
- the risks of poorly taken treatment are the worsening of the state of health, the risks of transmission of the virus during sexual intercourse without condoms, and the development by the virus of resistance to the treatment which can make it less effective,
- HIV infection permanently persists in the body; antiretroviral treatment should not be stopped, even when the viral load is undetectable. A person who takes their treatment well can live as long as an uncontaminated person;
- for professionals involved in the care of young patients living with HIV, an information sheet [5] summarizing the essence of the recommendations:
- general principles of antiretroviral treatment,
- pre-therapeutic assessment,
- criteria for choosing treatment,
- monitoring and support methods,
- management of therapeutic failure,
- prevention of bacterial and opportunistic infections,
- screening and prevention of hepatitis B and hepatitis C virus infections,
- cancer screening and prevention,
- vaccination, psychological and social care.
Antiretroviral treatment in children and adolescents: summary of recommendations
The recommended treatment is triple antiretroviral therapy comprising (cf. Painting):
- 2 nucleoside reverse transcriptase inhibitors (NRTI). As first-line treatment, zidovudine (ZDV), abacavir (ABC), lamivudine (3TC), tenofovir alafenamide (TAF), tenofovir disoproxil fumarate (TDF), or emtricitabine (FTC) are recommended;
- a third agent: an integrase inhibitor (INI) preferably, a non-nucleoside reverse transcriptase inhibitor (NNRTI) or a boosted protease inhibitor (PI). As first-line treatment, raltegravir (RAL), dolutegravir (DTG) or bictegravir (BIC) are recommended. Other possibilities are lopinavir + ritonavir (LPV/r), nevirapine (NVP), atazanavir + ritonavir (ATV/r), darunavir + ritonavir (DRV/r), doravirine (DOR), elvitegravir + cobicistat (EVG/c), efavirenz (EFV), and rilpivirine (RPV).
The criteria for choosing initial antiretroviral treatment are:
- the age of the patient: treatment should be considered in any child infected with HIV, and initiated as early as possible;
- the marketing authorization (AMM);
- the expected effectiveness, taking into account a risk of resistance (genotyping necessary);
- the existence of a suitable dosage form;
- the safety profile, i.e. the risk of potential adverse effects.
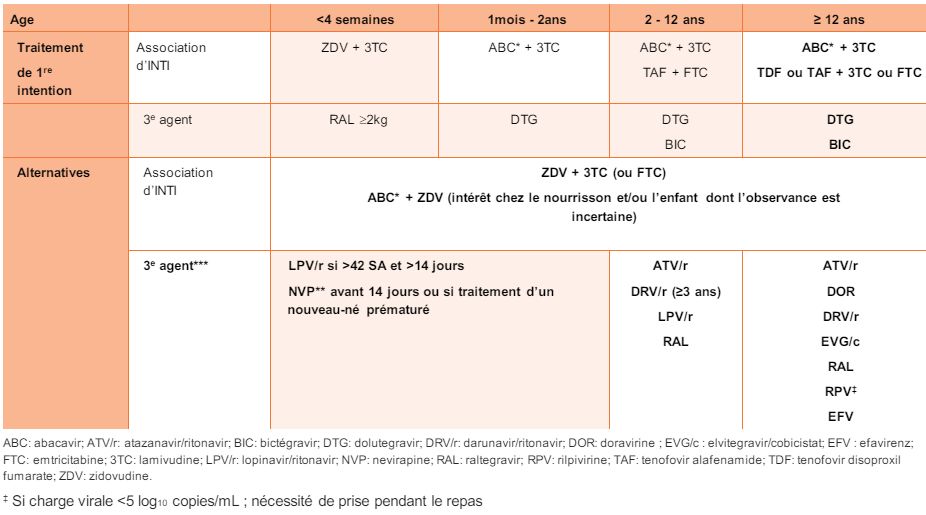
Table – Recommended antiretroviral treatment for children or adolescents living with HIV-1 in 1D intention and alternatives according to age (extract from the HAS recommendations [2])
*in the absence of HLA B*5701 (to be searched before any ABC prescription)
**avoid introducing NVP and ABC simultaneously
***advantages and disadvantages of 3e proposed alternative agent (cf. Annex 2 of the recommendations)
When prescribing or dispensing antiretroviral medications, doctors and pharmacists can refer to appendices 1 and 2 of the HAS recommendations:
- appendix 1: presentation in table form of dosage recommendations according to age, molecule by molecule;
- appendix 2: presentation of the advantages and disadvantages for each molecule, according to the galenic forms available:
- taste or size of the tablets,
- taken with food,
- number of doses per day,
- risk of hypersensitivity, renal, bone toxicity,
- risk of drug interactions,
- pharmacokinetic properties (half-life),
- experience in pediatrics.
Observance put to the test of everyday life
The HAS recommendations specify the monitoring methods and objectives of support for pediatric patients living with HIV, by a healthcare professional.
Monitoring the child or adolescent living with HIV must enable:
- to monitor the effectiveness and tolerance of the treatment, and to adapt it if necessary;
- to evaluate treatment compliance and identify factors for non-compliance;
- to adapt the treatment to the patient’s lifestyle:
- taking into account the advancing age of the patient: the adolescent period is at risk of non-compliance,
- by making adaptations to the treatment to better integrate it into daily life (schedules, vacations, dietary constraints);
- to simplify the intake diagram whenever possible:
- reduce the number of doses and tablets by using combined forms: favoring schedules with a single daily dose,
- consider DTG/3TC or DTG/RPV dual therapies on a case-by-case basis, or long-acting injectable treatments, under the same conditions as in adults.




{kind=link}