




Alain Guibeault arrives with his walker in his geriatrician’s office. He sits down, out of breath. Beep, beep, beep… The suction system, which helps the wound on one leg heal, is disconnected. The machine rings constantly.
Published at 5:00 a.m.
Beep beep beep. The Dre Julia Chabot checks the small pump. “She does that often?” ”, she asks. “In the night!” », replies Denise, Mr. Guibeault’s wife. “In the night?” It’s not supposed to ring, it’s supposed to suck. » The geriatrician examines the wound – it is “beautiful” – then contacts a nurse to adjust the machine.
This is one of the problems that the Dre Chabot will attempt to settle the matter during his consultation with Mr. Guibeault at the outpatient geriatrics clinic at St. Mary’s Hospital in Montreal. A 90-minute meeting (yes, yes, 90!) face-to-face, without a computer screen between the doctor and her patient.
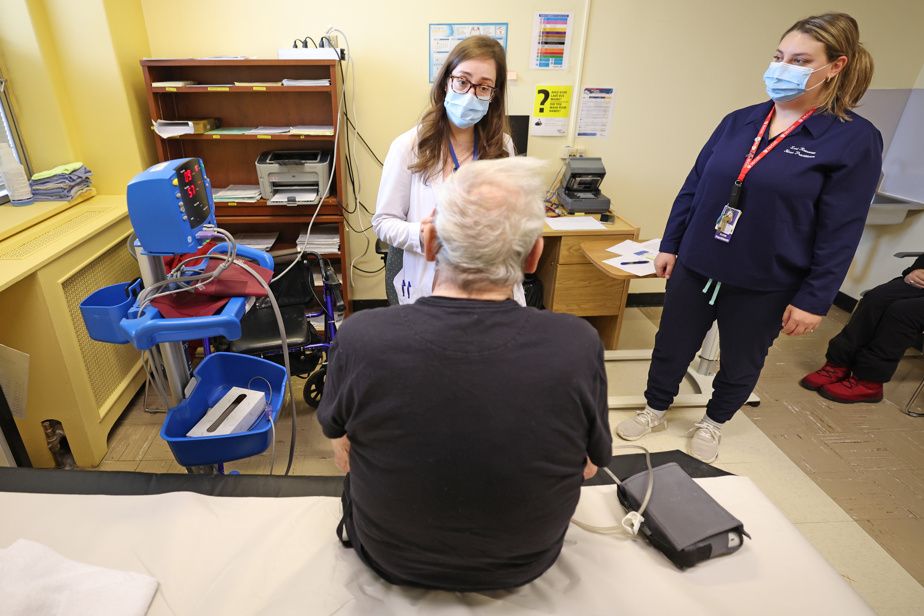
PHOTO ROBERT SKINNER, THE PRESS
Alain Guibeault, 77 years old, listens attentively to the Dre Julia Chabot.
“Geriatricians have a very holistic approach to patient care,” she explains.
During the consultation, the specialist reviews all aspects of her patient’s life: physical health problems, mood, medication, mobility, personal hygiene care, meal management, housekeeping, etc.
“It is certain that family doctors can do a lot of things and that many patients will never need to see a geriatrician in their life,” emphasizes the Dre Sculpin. But other “fragile” elderly people will need the expertise of this specialist. And there will be even more of them in the future with the aging of the population.
PHOTO ROBERT SKINNER, THE PRESS
The Dre Julia Chabot
It is certain that 148 geriatricians [au Québec]we won’t make it. There will need to be more of us and we will need occupational therapists, physiotherapists and social workers who have expertise in geriatrics.
The Dre Julia Chabot, geriatrician at St. Mary’s Hospital
Des cas complexes
Geriatricians see complex cases. Mr. Guibeault, 77 years old, takes around twenty pills a day. He suffers from chronic obstructive pulmonary disease, heart problems and shoulder pain. In 2024, he was hospitalized several times, notably to change his hip prosthesis which was causing him pain as well as for episodes of confusion linked to taking opioids aimed at reducing this pain.
In mid-December, a few days before the consultation, he had two falls at home. “I tripped over a lamp wire,” he said. And the second fall? “A dizzy spell. I fell on my butt because I protect my head a lot. Especially since I have a very good head,” he says jokingly.
PHOTO ROBERT SKINNER, THE PRESS
The Dre Julia Chabot examine son patient Alain Guibeault.
The Dre Chabot asks him to go to the stretcher to take his pressure while lying and standing to see if it drops. She rushes to give him her walker – her “Cadillac”, as she calls it.
“That’s the hardest step of the day: taking off the coat,” says Mr. Guibeault. His face tenses. His shoulders hurt terribly.
Check done, no pressure drop. The doctor suspects a medication may be contributing to the dizziness. She suggests stopping it, just like another one, which has become useless. From now on, Mr. Guibeault will take 21 pills rather than 23.
Concerns
Throughout the meeting, the Dre Chabot questions Denise. The latter says she is “fearful” because her partner forgot to turn off a stove ring on two occasions. The smoke detector went off.
Mr. Guibeault previously worked as a cook. Meals are his department. The Dre Chabot suggests making a request to the CLSC so that an occupational therapist can ensure that he cooks safely. He is not opposed to it, but refuses any meals on wheels. Just mentioning the possibility makes him roll his eyes.
PHOTO ROBERT SKINNER, THE PRESS
The Geriatric Care Unit at St. Mary’s Hospital
As her memory “plays tricks” on her in the kitchen, the geriatrician returns to the charge: “Put it on, your CPAP mask [traitement de ventilation à pression positive continue]to sleep? ” No. “I’d like you to try it,” said the D.re Sculpin. Maybe it would help your memory. »
His sleep and energy would improve. He falls asleep in the blink of an eye in front of the television, according to his wife. “If I was a sleeping pill, everyone would buy me!” “, he says playfully.
Another concern of Denise: Mr. Guibeault sometimes has visual hallucinations. The Dre Chabot explains that they can be generated by an infection. “Often older people have symptoms that can be very atypical,” she says. A blood test is taken on site. The results will later reveal an infection.
During the holiday season, Mr. Guibeault had to be hospitalized for pneumonia. “The hallucinations are gone,” he said to The Pressfrom his hospital bed. I still cough a little, but very little. » He must have his day off on Monday. “I hope it goes well. I wouldn’t want my wife to take all the trouble on her back. »
One thing is certain, he wants to stay away from the hospital in 2025. Even if he says he is “blessed” to have received good “personalized care” at St. Mary. “It’s a luxury to have a practically private geriatrician! »
A geriatrics team in the emergency room
PHOTO ROBERT SKINNER, THE PRESS
St. Mary’s Hospital Center
St. Mary’s Emergency Department has had its own geriatrics team for the past year. His mission? Reduce the length of seniors’ stays in emergency rooms and avoid hospitalizations. Early in the morning, a nurse targets elderly patients who need to be evaluated as a priority. A geriatrician, an occupational therapist, a physiotherapist or a social worker takes care of them. If the patient’s condition allows it, the team already organizes his discharge. “Sometimes a patient has a fracture, is medically stable and just needs a post-acute bed [en réadaptation]says Leeza Paolone, clinical nurse. We make the request from the emergency. » The team has seen 1,200 patients so far. “We gave around 300 leaves of absence,” says the Dre Julia Chabot.



